Modern bariatric surgery offers several treatment options for severe obesity, and each method has its own objectives, limitations and expected outcomes. That said, mini-gastric bypass is currently considered one of the most effective options when the aim is not only to help the patient lose weight but also to address metabolic disorders. The method combines significant weight loss with metabolic effects, which is why it is often considered for people with type 2 diabetes, insulin resistance and other obesity-related complications.
Despite the prefix ‘mini’, this is a major surgical procedure, not a ‘light version’ of bariatric surgery. The name is linked to the technical specifics: in OAGB, a single anastomosis is created, but the operation itself delivers powerful and stable results and requires the same level of thorough preparation, monitoring and lifestyle changes as other bypass methods. This is precisely why it is particularly important to view mini-gastric bypass not as a quick way to lose weight, but as a powerful treatment tool for patients with obesity and associated metabolic disorders.
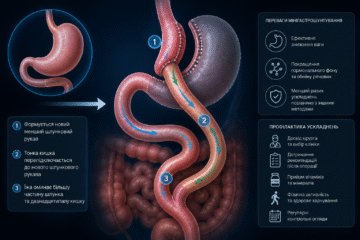
What is mini-gastric bypass surgery and what is the essence of the method
Mini-gastric bypass is a bariatric procedure in which the surgeon creates a long, narrow tube from the stomach with a capacity of around 50 ml, and then connects it to the small intestine. As a result, the method works in two ways simultaneously. The first mechanism is restrictive: the patient feels full more quickly and is physically unable to eat large quantities of food. The second is malabsorptive: part of the small intestine is bypassed in the normal digestive process, so the absorption of some fats and carbohydrates is reduced. Put simply, the patient eats less, and the body absorbs fewer calories from food than before.
The method is called ‘mini’ not because the operation is simple or minor, but because of the specific nature of the technique. Unlike classic gastric bypass surgery, here only a single anastomosis is created – a single connection between the stomach and the intestine – whereas with Roux-en-Y there are two such connections. It is precisely this approach that makes the procedure technically less complex, potentially shortening the duration of the operation and reducing some of the intraoperative risks whilst maintaining a significant effect on weight loss and metabolic control. Therefore, mini-gastric bypass is regarded as a serious yet straightforward method for treating obesity and associated metabolic disorders.
Main indications: who is suitable for this operation
Mini-gastric bypass surgery is not prescribed simply because a patient wishes to ‘lose weight faster’, but according to clear medical criteria. Primarily, this concerns patients with a BMI of 40 or higher, as well as those with a BMI of 35 or higher if they have obesity-related complications. This method is particularly important for people with type 2 diabetes and metabolic syndrome, because bypass surgery can improve carbohydrate metabolism within the first few days and weeks after the procedure, even before significant weight loss occurs. This is precisely why such surgery is viewed not only as a means of reducing body weight, but also as a tool for addressing serious metabolic disorders. The main indications usually include the following situations:
- A BMI of 40 kg/m² or higher, even if associated complications have not yet reached a severe stage.
- A BMI of 35 kg/m² or above in the presence of obesity-related conditions, including type 2 diabetes, high blood pressure, obstructive sleep apnoea and other metabolic disorders.
- Type 2 diabetes and severe metabolic syndrome, where the aim is not only to achieve weight loss but also a sustained improvement in glucose control.
- Failure of a previous bariatric operation, for example following gastric banding or sleeve gastrectomy, if weight has been regained or the expected outcome has proved insufficient. In such cases, OAGB may be considered as a repeat procedure.
It is worth mentioning repeat operations separately. If the previous procedure did not produce the desired result, this does not always mean that surgical treatment has exhausted its possibilities. In some cases, mini-gastric bypass is used as a revision procedure following ineffective gastric banding or sleeve gastrectomy to enhance weight loss and achieve a more pronounced metabolic effect. Therefore, the final decision is always made following a face-to-face assessment of the patient’s condition, treatment history and risks, rather than solely on the basis of the figure on the scales.
Possible complications and their prevention
Any bariatric surgery naturally raises questions in the patient’s mind about the risks, and mini-gastric bypass is no exception. It is important to discuss complications honestly but calmly: most problems can be prevented by following the surgeon’s recommendations and not neglecting post-operative follow-up. One specific condition following bypass surgery is dumping syndrome. It can manifest as sudden weakness, sweating, nausea, palpitations and discomfort after eating sweet or very fatty foods. It sounds unpleasant, but in essence it is a kind of ‘safety mechanism’ that helps the patient adjust their diet more quickly and avoid foods that hinder recovery. Here is what is particularly important for preventing complications after surgery:
- avoid sugary drinks, desserts, fried and very fatty foods to reduce the risk of dumping syndrome and make the adaptation phase easier;
- give up smoking completely, as it increases the risk of ulcers in the anastomosis area;
- take proton pump inhibitors and other medications strictly as prescribed during the healing period;
- do not miss follow-up appointments and inform your doctor immediately of any pain, nausea, vomiting or severe weakness after eating.
The risk of an anastomotic ulcer – a sore at the junction of the stomach and intestine – requires particular attention. This is precisely why it is so important to be monitored by a specialist. Our Avicenna Med clinic offers comprehensive patient support at all stages of treatment, so it is advisable to consult a bariatric surgeon both before the operation and during the post-operative period. This approach helps to assess risk factors in advance, select the appropriate preventive measures, and make recovery after mini-gastric bypass surgery safer and more predictable.
Life after surgery: diet and addressing nutritional deficiencies
Life changes quite rapidly after surgery: meals become more frequent, portions smaller, and eating habits more mindful. In the first month, the diet is expanded in stages: first, liquids are permitted, then puréed food, followed by soft foods, and only then are more solid foods gradually introduced. This transition is necessary to allow the stomach and the area where it connects to the intestine to heal properly. Mini-gastric bypass surgery requires careful adaptation rather than rushing: you need to eat slowly, chew your food thoroughly and, from the very first weeks, focus on getting enough protein, as this is what helps maintain muscle mass and makes the weight loss period easier to manage.
An equally important part of life after surgery is lifelong management of nutrient deficiencies. As part of the intestine where certain nutrients are absorbed functions differently following the bypass procedure, patients usually require ongoing intake of special bariatric vitamin and mineral supplements, as well as iron, calcium and vitamin B12, as prescribed by their doctor. Even if you feel well, such supplements should not be considered a temporary measure: following mini-gastric bypass surgery, they become part of long-term health management, alongside regular tests and dosage adjustments. It is precisely this approach that helps prevent anaemia, weakness, reduced bone density and other consequences of hidden deficiencies.
Mini-gastric bypass surgery at the Avicenna Med clinic
At our Avicenna Med clinic, mini-gastric bypass surgery is performed laparoscopically – via several small incisions – under general anaesthesia. This method of surgery helps to minimise tissue trauma and makes recovery more comfortable for the patient. Safety depends not only on the surgeon’s skill but also on the environment in which the operation takes place; therefore, at Avicenna Med, we place great emphasis on state-of-the-art facilities: the clinic boasts operating theatres, an intensive care unit and a high-comfort ward where patients can be monitored following the procedure.
It is equally important to note that treatment does not end on the day of discharge. At Avicenna Med, our bariatric programme includes post-operative care, and prior to the procedure, patients can undergo diagnostic tests and have blood tests carried out in a single location. Long-term monitoring is particularly important following bypass surgery: bariatric guidelines require regular monitoring of test results, tracking of deficiencies and adjustment of vitamin, iron, calcium and B12 dosages, and annual visits to a specialist are necessary throughout a patient’s life. It is precisely this approach that makes the outcome of the surgery not only noticeable but also manageable in the long term.
Conclusion
Mini-gastric bypass surgery can be a significant step towards weight loss and improved health, but it is important to understand that the surgery does not work on its own and does not replace the patient’s active participation in their own treatment. It is a powerful tool that delivers results when combined with discipline, adherence to the doctor’s recommendations, and a willingness to change eating habits for the long term. That is precisely why you should not start with doubts, but with a professional assessment of your physical condition – book a consultation at our Avicenna Med clinic so that a doctor can assess your situation, take any underlying conditions into account, and help you choose the most suitable type of bariatric surgery.
FAQ
- How long does recovery take after mini-gastric bypass surgery?
The first few days are spent adapting to drinking, walking and pain management. Then a gradual reintroduction of food begins. Most patients transition to a more familiar food texture gradually over several weeks, and to a normal diet after about 6–8 weeks, provided healing proceeds smoothly.
- Can you manage without vitamins if your diet has become ‘perfect’?
No. Following bariatric bypass surgery, even a good diet alone does not eliminate the risk of deficiencies. Post-operative management guidelines recommend regular intake of vitamin B12, iron, calcium, vitamin D and other supplements, depending on the type of surgery and test results.
- How does mini-gastric bypass differ from classic gastric bypass?
The main difference lies in the number of anastomoses. In mini-gastric bypass surgery, a single connection is created between the stomach and the intestine, whereas in classic Roux-en-Y surgery, two are created. As a result, the operation can be technically simpler and shorter, whilst the mechanism of action remains powerful: reduced food volume, reduced absorption of some calories and a pronounced metabolic effect.